Human Hands And Legs
Hand

Humans have two hands located at the distal end of each arm. Apes and monkeys are sometimes described as having four hands, because the toes are long and the hallux is opposable and looks more like a thumb, thus enabling the feet to be used as hands. Also, some apes have toes that are longer than human fingers. The word "hand" is sometimes used by evolutionary anatomists to refer to the appendage of digits on the forelimb such as when researching the homology between the three digits of the bird hand and the dinosaur hand.
Human anatomy
The human hand consists of a broad palm (metacarpus) with 5 digits, attached to the forearm by a joint called the wrist (carpus). The back of the hand is formally called the opisthenar.
Digits
The four fingers on the hand are used for the outermost performance; these four digits can be folded over the palm which allows the grasping of objects. Each finger, starting with the one closest to the thumb, has a colloquial name to distinguish it from the others:
Human anatomy
The human hand consists of a broad palm (metacarpus) with 5 digits, attached to the forearm by a joint called the wrist (carpus). The back of the hand is formally called the opisthenar.
Digits
The four fingers on the hand are used for the outermost performance; these four digits can be folded over the palm which allows the grasping of objects. Each finger, starting with the one closest to the thumb, has a colloquial name to distinguish it from the others:
- index finger (digitus secundus manus), pointer finger, or forefinger
- middle finger (digitus médius and more commonly digitus tertius)
- ring finger (digitus annuláris) - annulus
- little finger (digitus mínimus mánus) or 'pinky' - minimus
Structure Of Hand
Bones of hand
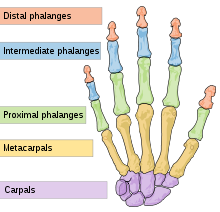
The human hand has 27 bones: the carpus or wrist accounts for 8; the metacarpals or palm contains five; the remaining fourteen are digital bones; fingers and thumb
The eight bones of the wrist are arranged in two rows of four. These bones fit into a shallow socket formed by the bones of the forearm. The bones of proximal row are (from lateral to medial): scaphoid, lunate, triquetral and pisiform. The bones of the distal row are (from lateral to medial): trapezium, trapezoid, capitate and hamate. An easy way to remember them all is with the mnemonic.
The palm has five bones known as metacarpal bones, one to each of the 5 digits. These metacarpals have a head, a shaft, and a base.
Human hands contain fourteen digital bones, also called phalanges, or phalanx bones: two in the thumb (the thumb has no middle phalanx) and three in each of the four fingers. These are the distal phalanx, carrying the nail, the middle phalanx, and the proximal phalanx.
Sesamoid bones are small ossified nodes embedded in the tendons to provide extra leverage and reduce pressure on the underlying tissue. Many exist around the palm at the bases of the digits; the exact number varies between different people.
Articulations
The articulation of the human hand is more complex and delicate than that of comparable organs in any other animal. Without this extra articulation, we would not be able to operate a wide variety of tools and devices, nor achieve the wide variety of possible hand gestures.
The articulations are:
The eight bones of the wrist are arranged in two rows of four. These bones fit into a shallow socket formed by the bones of the forearm. The bones of proximal row are (from lateral to medial): scaphoid, lunate, triquetral and pisiform. The bones of the distal row are (from lateral to medial): trapezium, trapezoid, capitate and hamate. An easy way to remember them all is with the mnemonic.
The palm has five bones known as metacarpal bones, one to each of the 5 digits. These metacarpals have a head, a shaft, and a base.
Human hands contain fourteen digital bones, also called phalanges, or phalanx bones: two in the thumb (the thumb has no middle phalanx) and three in each of the four fingers. These are the distal phalanx, carrying the nail, the middle phalanx, and the proximal phalanx.
Sesamoid bones are small ossified nodes embedded in the tendons to provide extra leverage and reduce pressure on the underlying tissue. Many exist around the palm at the bases of the digits; the exact number varies between different people.
Articulations
The articulation of the human hand is more complex and delicate than that of comparable organs in any other animal. Without this extra articulation, we would not be able to operate a wide variety of tools and devices, nor achieve the wide variety of possible hand gestures.
The articulations are:
- interphalangeal articulations of hand (the hinge joints between the finger bones)
- metacarpophalangeal joints (where the fingers meet the palm)
- intercarpal articulations (where the palm meets the wrist)
- wrist (may also be viewed as belonging to the forearm.)
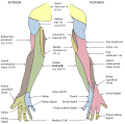
Muscles

The muscles acting on the hand can be subdivided into two groups: the extrinsic and intrinsic muscle groups. The extrinsic muscle groups are the long flexors and extensors. They are called extrinsic because the muscle belly is located on the forearm.
Intrinsic
The intrinsic muscle groups are the thenar (thumb) and hypothenar (little finger) muscles; the interossei muscles (four dorsally and three volarly) originating between the metacarpal bones; and the lumbrical muscles arising from the deep flexor (and are special because they have no bony origin) to insert on the dorsal extensor hood mechanism.
Extrinsic
The fingers have two long flexors, located on the underside of the forearm. They insert by tendons to the phalanges of the fingers. The deep flexor attaches to the distal phalanx, and the superficial flexor attaches to the middle phalanx. The flexors allow for the actual bending of the fingers. The thumb has one long flexor and a short flexor in the thenar muscle group. The human thumb also has other muscles in the thenar group (opponens and abductor brevis muscle), moving the thumb in opposition, making grasping possible.
The extensors are located on the back of the forearm and are connected in a more complex way than the flexors to the dorsum of the fingers. The tendons unite with the interosseous and lumbrical muscles to form the extensorhood mechanism. The primary function of the extensors is to straighten out the digits. The thumb has two extensors in the forearm; the tendons of these form the anatomical snuff box. Also, the index finger and the little finger have an extra extensor, used for instance for pointing. The extensors are situated within 6 separate compartments.
Disorders and diseases
Fractures of the hand include:
Intrinsic
The intrinsic muscle groups are the thenar (thumb) and hypothenar (little finger) muscles; the interossei muscles (four dorsally and three volarly) originating between the metacarpal bones; and the lumbrical muscles arising from the deep flexor (and are special because they have no bony origin) to insert on the dorsal extensor hood mechanism.
Extrinsic
The fingers have two long flexors, located on the underside of the forearm. They insert by tendons to the phalanges of the fingers. The deep flexor attaches to the distal phalanx, and the superficial flexor attaches to the middle phalanx. The flexors allow for the actual bending of the fingers. The thumb has one long flexor and a short flexor in the thenar muscle group. The human thumb also has other muscles in the thenar group (opponens and abductor brevis muscle), moving the thumb in opposition, making grasping possible.
The extensors are located on the back of the forearm and are connected in a more complex way than the flexors to the dorsum of the fingers. The tendons unite with the interosseous and lumbrical muscles to form the extensorhood mechanism. The primary function of the extensors is to straighten out the digits. The thumb has two extensors in the forearm; the tendons of these form the anatomical snuff box. Also, the index finger and the little finger have an extra extensor, used for instance for pointing. The extensors are situated within 6 separate compartments.
Disorders and diseases
- Polymelia, a birth defect in which the individual has more than the usual number of limbs. Amelia, a congenital absence of limbs
- Polydactyly, more than the usual number of fingers or toes. Having more than the typical number of metacarpal bones may be caused by genetic disorders like Catel-Manzke syndrome.
- Syndactyly, fusion of fingers or toes.
- Hand infection
- Hand surgery
- Carpal Tunnel Syndrome
- Dupuytren's Contracture
- Claw hand, paralysis of intrinsic muscles of hand.
Fractures of the hand include:
- Scaphoid fracture
- Rolando fracture - a comminuted intra-articular fracture through the base of the first metacarpal bone
- Bennett's fracture - a fracture of the base of the first metacarpal bone which extends into the carpometacarpal (CMC) joint. Boxer's fracture - a fracture at the neck of a metacarpal
Legs
The human leg is the entire lower extremity or limb of the human body, including the foot, thigh and even the hip or gluteal region, only to the section of the lower limb extending from the knee to the ankle. Legs are used for standing, walking, jumping, running, kicking, and similar activities, and constitute a significant portion of a person's mass.
Anatomy
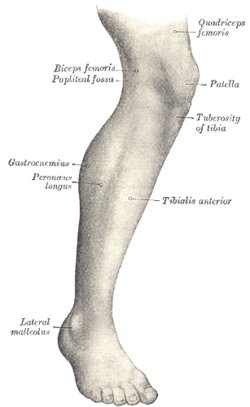
In human anatomical terms, the leg is the part of the lower limb that lies between the knee and the ankle, the thigh is between the hip and knee and the term "lower limb" is used to describe the colloquial leg. This article generally follows the common usage.
The leg from the knee to the ankle is called the cnemis or crus. The calf is the back portion and the shin is the front.
Evolution has provided the human body with two distinct features: the specialization of the upper limb for visually guided manipulation and the lower limb's development into a mechanism specifically adapted for efficient bipedal gait. While the capacity to walk upright is not unique to humans, other primates can only achieve this for short periods and at a great expenditure of energy. The human adaption to bipedalism is not limited to the leg, however, but has also affected the location of the body's center of gravity, the reorganisation of internal organs, and the form and biomechanism of the trunk. In humans, the double S-shaped vertebral column acts as a shock-absorber which shifts the weight from the trunk over the load-bearing surface of the feet. The human legs are exceptionally long and powerful as a result of their exclusive specialization to support and locomotion — in orangutans the leg length is 111% of the trunk; in chimpanzees 128%, and in humans 171%. Many of the leg's muscles are also adapted to bipedalism, most substantially the gluteal muscles, the extensors of the knee joint, and the calf muscles.
The leg from the knee to the ankle is called the cnemis or crus. The calf is the back portion and the shin is the front.
Evolution has provided the human body with two distinct features: the specialization of the upper limb for visually guided manipulation and the lower limb's development into a mechanism specifically adapted for efficient bipedal gait. While the capacity to walk upright is not unique to humans, other primates can only achieve this for short periods and at a great expenditure of energy. The human adaption to bipedalism is not limited to the leg, however, but has also affected the location of the body's center of gravity, the reorganisation of internal organs, and the form and biomechanism of the trunk. In humans, the double S-shaped vertebral column acts as a shock-absorber which shifts the weight from the trunk over the load-bearing surface of the feet. The human legs are exceptionally long and powerful as a result of their exclusive specialization to support and locomotion — in orangutans the leg length is 111% of the trunk; in chimpanzees 128%, and in humans 171%. Many of the leg's muscles are also adapted to bipedalism, most substantially the gluteal muscles, the extensors of the knee joint, and the calf muscles.
Bones
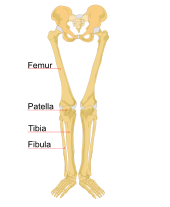
The major (long) bones of the human leg are the femur (thighbone), tibia (shinbone), and fibula (the smaller, rear calf bone). The patella (kneecap) is the bone in front of the knee. Most of the leg skeleton has bony prominences and margins that can be palpated, notable exceptions being the hip joint, and the neck and shaft of femur. Many of these anatomical landmarks are used to define the extent of the leg: most notably the anterior superior iliac spine, the greater trochanter, the superior margin of the medial condyle of tibia, and the medial malleolus.
In the normal case, the large joints of the lower limb are aligned on a straight line which represents the mechanical longitudinal axis of the leg, the Mikulicz line. This line stretches from the hip joint (or more precisely the head of the femur), through the knee joint (the intercondylar eminence of the tibia), and down to the center of the ankle (the ankle mortise, the fork-like grip between the medial and lateral malleoli). In the tibial shaft, the mechanical and anatomical axes coincide, but in the femoral shaft they diverge 6°, resulting in the femorotibial angle of 174° in a leg with normal axial alignment.
A leg is considered straight when, with the feet brought together, both the medial malleoli of the ankle and the medial condyles of the knee are touching. Divergence from the normal femorotibial angle is called genu varum if the center of the knee joint is lateral to the mechanical axis (intermalleolar distance exceeds 3 cm), and genu valgum if it is medial to the mechanical axis (intercondylar distance exceeds 5 cm). These conditions impose unbalanced loads on the joints and stretching of either the thigh's adductors and abductors. The angle of inclination formed between the neck and shaft of the femur, the collodiaphysial angle, varies with age—about 150° in the newborn, it gradually decreases to 126-128° in adults, to reach 120° in old age. Pathological changes in this angle results in abnormal posture of the leg:
A small angle produces coxa vara and a large angle in coxa valga; the latter is usually combined with genu varum and coxa vara leads genu valgum. Additionally, a line drawn through the femoral neck superimposed on a line drawn through the femoral condyles forms an angle, the torsion angle, which makes it possible for flexion movements of the hip joint to be transposed into rotary movements of the femoral head. Abnormally increased torsion angles results in a limb turned inward and a decreased angle in a limb turned outward; both cases resulting in a reduced range of mobility.
In the normal case, the large joints of the lower limb are aligned on a straight line which represents the mechanical longitudinal axis of the leg, the Mikulicz line. This line stretches from the hip joint (or more precisely the head of the femur), through the knee joint (the intercondylar eminence of the tibia), and down to the center of the ankle (the ankle mortise, the fork-like grip between the medial and lateral malleoli). In the tibial shaft, the mechanical and anatomical axes coincide, but in the femoral shaft they diverge 6°, resulting in the femorotibial angle of 174° in a leg with normal axial alignment.
A leg is considered straight when, with the feet brought together, both the medial malleoli of the ankle and the medial condyles of the knee are touching. Divergence from the normal femorotibial angle is called genu varum if the center of the knee joint is lateral to the mechanical axis (intermalleolar distance exceeds 3 cm), and genu valgum if it is medial to the mechanical axis (intercondylar distance exceeds 5 cm). These conditions impose unbalanced loads on the joints and stretching of either the thigh's adductors and abductors. The angle of inclination formed between the neck and shaft of the femur, the collodiaphysial angle, varies with age—about 150° in the newborn, it gradually decreases to 126-128° in adults, to reach 120° in old age. Pathological changes in this angle results in abnormal posture of the leg:
A small angle produces coxa vara and a large angle in coxa valga; the latter is usually combined with genu varum and coxa vara leads genu valgum. Additionally, a line drawn through the femoral neck superimposed on a line drawn through the femoral condyles forms an angle, the torsion angle, which makes it possible for flexion movements of the hip joint to be transposed into rotary movements of the femoral head. Abnormally increased torsion angles results in a limb turned inward and a decreased angle in a limb turned outward; both cases resulting in a reduced range of mobility.
Vein

The veins are subdivided into three systems. The deep or epifascial system returns approximately 85 percent of the blood and the superficial or intermuscular system approximately 15 percent. A series of venous valves called the perforating system interconnects the superficial and deep systems. In the standing posture, the veins of the leg have to handle an exceptional load as they act against gravity when they return the blood to the heart. The venous valves assist in maintaining the superficial-to-deep direction of the blood flow.
Greater saphenous vein
Nerves of right leg, anterior and posterior aspects
The sensory and motor innervation to the lower limb is supplied by the lumbosacral plexus, which is formed by the ventral rami of the lumbar and sacral spinal nerves with additional contributions from the subcostal nerve (T12) and coccygeal nerve (Co1). Based on distribution and topography, the lumbosacral plexus is subdivided into the lumbar plexus (T12-L4) and the Sacral plexus (L5-S4); the latter is often further subdivided into the sciatic and pudendal plexuses:
Greater saphenous vein
- Small saphenous
- Femoral vein
- Popliteal vein
- Anterior tibial vein
- Posterior tibial vein
- Fibular vein
Nerves of right leg, anterior and posterior aspects
The sensory and motor innervation to the lower limb is supplied by the lumbosacral plexus, which is formed by the ventral rami of the lumbar and sacral spinal nerves with additional contributions from the subcostal nerve (T12) and coccygeal nerve (Co1). Based on distribution and topography, the lumbosacral plexus is subdivided into the lumbar plexus (T12-L4) and the Sacral plexus (L5-S4); the latter is often further subdivided into the sciatic and pudendal plexuses:
- The lumbar plexus is formed lateral to the intervertebral foramina by the ventral rami of the first four lumbar spinal nerves, which all pass through psoas major.
- The nerves of the sacral plexus pass behind the hip joint to innervate the posterior part of the thigh, most of the lower leg, and the foot.
